Craniectomy for Clot (Evacuation of subdural hematoma) Neurosurgery
Craniectomy for clot is a brain surgery to remove a subdural hematoma, which is a collection of blood between the brain and its outer covering.
Overview
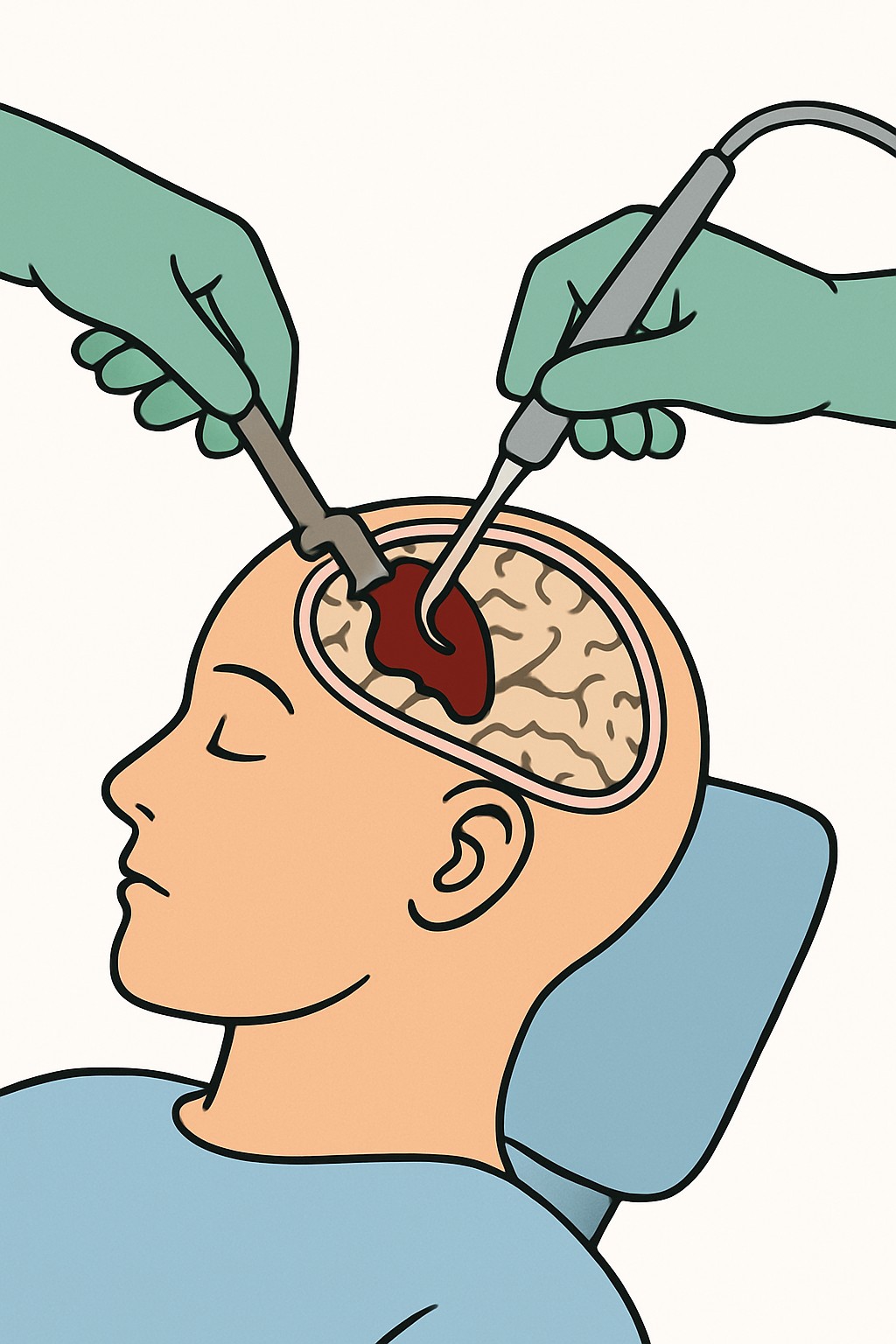
Craniectomy for clot is a brain surgery to remove a subdural hematoma, which is a collection of blood between the brain and its outer covering. The surgeon removes a section of skull to access the clot, clears the blood, and relieves pressure on the brain. In a craniectomy, the bone piece may be left off temporarily to allow the brain to swell safely. This procedure is often urgent when the hematoma is large, causing symptoms, or compressing the brain. A small drain may be placed to remove leftover fluid. Later, a separate surgery called cranioplasty may replace the bone or place a custom implant.
Also known as: SDH evacuation, Decompressive craniectomy for SDH, Subdural clot removal
Preparation & Next Steps
Everything you need to know before and after your procedure
Before Care
- Expect urgent brain imaging such as CT to confirm the size and location of the hematoma
- Share a current list of medicines, especially blood thinners and antiplatelet drugs, and known allergies
- Blood tests are commonly done to check blood counts and clotting status
- Follow any instructions about not eating or drinking before anesthesia if time allows
- Remove jewelry and hair accessories and bring photo ID and insurance information if available
- Identify a health care decision-maker and bring any advance directive documents
- Plan for a hospital and possible ICU stay and arrange support at home for early recovery
- Pack basic items only and avoid valuables
- Ask what to expect about drains, the bone flap, and the possibility of later cranioplasty
After Care
- Hospital care often starts in the ICU with frequent neurologic checks and monitoring
- Keep the incision clean and dry as instructed and do not apply lotions or creams unless told by the team
- A head dressing and surgical drain may be used for a short period and are managed by the care team
- Medicines may include pain control and seizure prevention; take them exactly as directed by your clinicians
- Increase activity gradually with guidance from physical and occupational therapy
- Protect the area without a bone flap from bumps; use any provided protective covering as instructed
- Schedule and attend follow-up visits for wound check, suture or staple removal, and repeat imaging if planned
- Watch for concerning signs such as worsening headache, confusion, new weakness or numbness, speech changes, seizures, fever, or drainage from the incision and contact a clinician
- Discuss when it is appropriate to return to driving, work, and strenuous activities
- Follow the plan to prevent constipation and stay hydrated and nourished during recovery
Clinical Information
Important medical details about this procedure
Indications
- Acute or chronic subdural hematoma with neurologic symptoms
- Large hematoma with mass effect or midline shift on imaging
- Rapid clinical decline or increased pressure inside the skull
- Failure of nonoperative management or less invasive drainage
- Recurrent subdural hematoma after prior treatment
- Need for decompression when brain swelling is expected
Alternatives
- Observation with serial imaging when appropriate
- Reversal or adjustment of blood thinners
- Burr hole drainage or twist-drill craniostomy for select chronic SDH
- Craniotomy with clot evacuation and bone flap replacement
- Palliative or comfort-focused care based on goals
Risks
- Bleeding or reaccumulation of the hematoma
- Infection of the wound or bone
- Seizures
- Stroke or brain swelling
- Neurologic deficits such as weakness, speech, or memory changes
- Cerebrospinal fluid leak
- Need for repeat surgery, including later cranioplasty
- Anesthesia-related complications
Contraindications
- Uncontrolled bleeding disorders without available reversal
- Severe medical instability where surgical risk outweighs potential benefit
- Care goals that do not include aggressive neurosurgical treatment
Recovery Timeline
What to expect during your recovery
Recovery varies by the size of the bleed, brain swelling, age, and other injuries. Hospitalization is often days to weeks, and rehabilitation can continue for weeks to months.
Typical Range
14–90 days
Return to Work
30–180 days
Recovery Milestones
ICU monitoring; sit up and stand with assistance as tolerated
Walk short distances with assistance; begin basic self-care
Suture or staple removal if planned; increase light daily activities
Gradual increase in walking and household tasks; continue therapy
Evaluate readiness for light work and driving based on recovery and clinical guidance
Frequently Asked Questions
Common questions and expert answers about this procedure
What is the difference between craniectomy and craniotomy?
What is the difference between craniectomy and craniotomy?
In a craniectomy the bone piece is left off temporarily to allow room for swelling. In a craniotomy the bone flap is replaced at the end of surgery.
Why is this surgery done for a subdural hematoma?
Why is this surgery done for a subdural hematoma?
It removes blood that is pressing on the brain and lowers pressure inside the skull, which can help limit further brain injury.
Will the bone be replaced later?
Will the bone be replaced later?
Many people have a later procedure called cranioplasty to replace the bone or place an implant. Timing depends on recovery and imaging.
How long does the operation take?
How long does the operation take?
Time varies with the size and complexity of the hematoma and whether swelling is present. It often lasts several hours including anesthesia and setup.
Will I have a drain?
Will I have a drain?
A small drain is often used for a short time to remove blood or fluid and reduce the chance of fluid build-up.
How long is the hospital stay?
How long is the hospital stay?
Many people spend time in the ICU first, then move to a regular unit. The total stay varies from several days to longer if rehabilitation is needed.
Can the hematoma come back?
Can the hematoma come back?
Yes, subdural hematomas can recur, especially in older adults or when on blood thinners. Some people need additional drainage or surgery.
Will I need rehabilitation?
Will I need rehabilitation?
Physical, occupational, and speech therapy are common to help with strength, balance, thinking, and daily activities.
References
Medical literature and sources