Spinal Fusion (Lumbar) Orthopedic Surgery
Lumbar spinal fusion is a surgery that joins two or more bones of the lower back (vertebrae) so they heal into one solid bone.
Overview
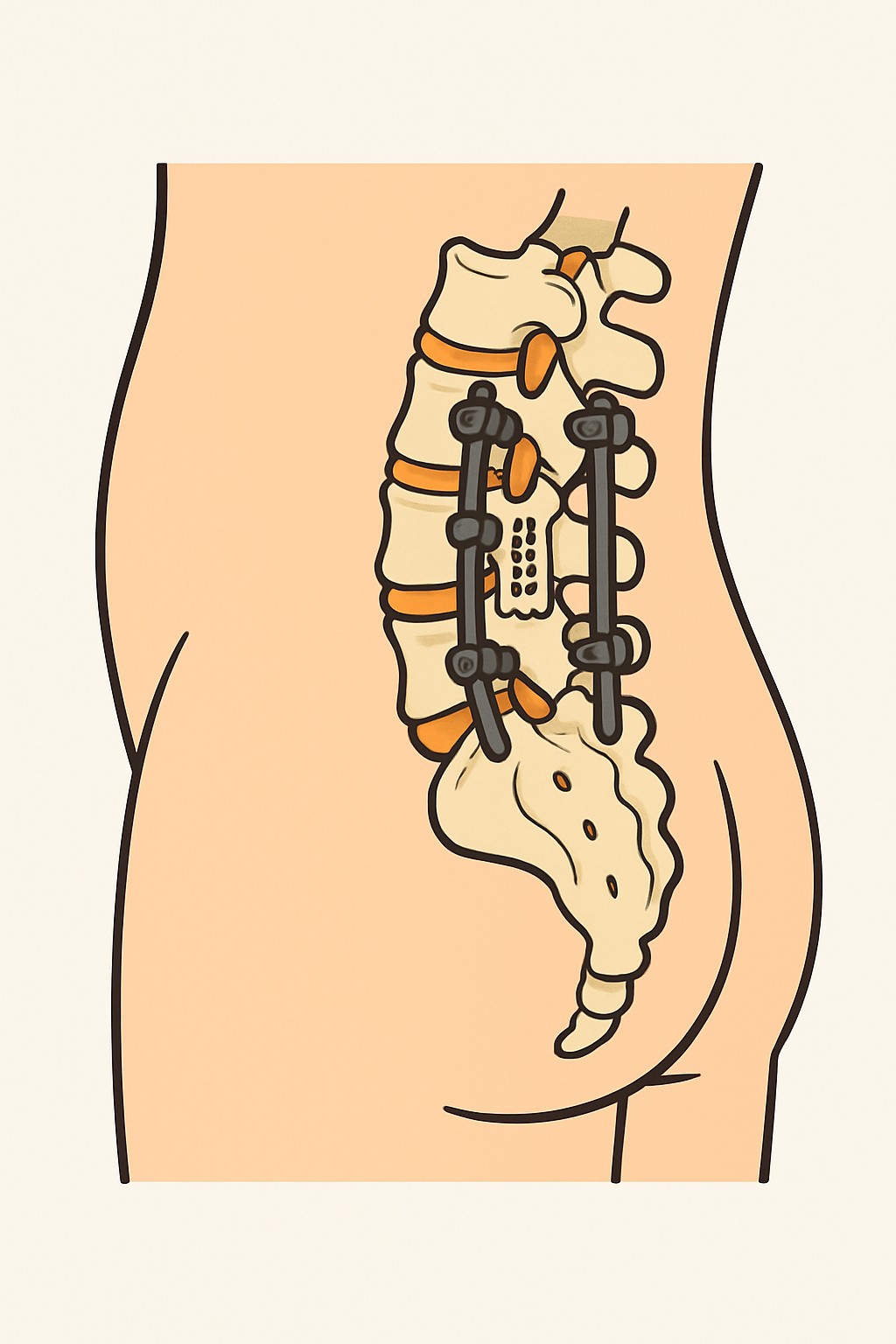
Lumbar spinal fusion is a surgery that joins two or more bones of the lower back (vertebrae) so they heal into one solid bone. Surgeons place bone graft between the vertebrae and often add screws, rods, or cages to hold the spine steady while the bone heals. It is done to reduce painful motion and stabilize the spine when there is instability, deformity, or damage. Recovery focuses first on safe movement and wound care, then on gradual return to activity while the bone fusion strengthens over time.
Also known as: Lumbar fusion, Lumbar spinal fusion, Lower back fusion
Preparation & Next Steps
Everything you need to know before and after your procedure
Before Care
- Attend the preoperative visit to review the plan, levels to be fused, consent, and expected hospital stay
- Share a complete list of medicines and supplements; ask how to manage blood thinners, diabetes medicines, and herbal products before surgery
- Complete ordered testing such as bloodwork, ECG, and updated spine imaging
- Discuss smoking and nicotine; nicotine can slow bone healing and increase complications
- Arrange a ride home and someone to help with daily tasks for the first few days
- Prepare your home by clearing tripping hazards, setting up a comfortable sleeping area, and stocking easy meals and supplies
- Plan time away from work, school, and caregiving duties based on your surgical team’s general guidance
- Follow specific fasting instructions and morning-of-surgery medicine directions provided by your surgical team
- If given a brace or walker, bring it on the day of surgery and wear loose, comfortable clothing
- Discuss bone graft options (your own bone, donor bone, or synthetic) and the rehabilitation plan after surgery
After Care
- Keep the incision clean and dry; follow instructions for dressing changes and showering
- Take pain medicines only as directed and store them safely; ask about non-medicine pain strategies
- Walk short, frequent distances each day and increase gradually as advised
- Avoid bending, twisting, and heavy lifting until your surgical team clears these activities
- Use any brace or walker as prescribed to support healing and safety
- Prevent constipation by staying hydrated, eating fiber, and using stool softeners if recommended
- Do not drive until your surgical team says it is safe and you are not taking opioid pain medicines
- Avoid tobacco and nicotine products because they can slow bone healing
- Attend follow-up visits and any ordered imaging to check hardware position and fusion progress
- Contact your surgical team for fever, increasing redness, swelling, drainage, worsening pain, new numbness or weakness, trouble walking, or new bladder or bowel problems
Clinical Information
Important medical details about this procedure
Indications
- Spinal instability from spondylolisthesis (vertebra slipping)
- Degenerative disc disease with instability and persistent pain
- Lumbar spinal stenosis with instability after decompression
- Recurrent or large disc herniation needing stabilization
- Spinal deformity such as scoliosis or kyphosis
- Fracture, infection, or tumor requiring stabilization
Alternatives
- Physical therapy and exercise program
- Pain management medicines
- Epidural steroid injections or nerve blocks
- Activity modification and weight management
- Cognitive behavioral therapy for chronic pain
- Decompression surgery without fusion when the spine is stable
- Spinal cord stimulation for select chronic pain cases
Risks
- Infection or poor wound healing
- Bleeding or blood clots
- Nerve injury, weakness, numbness, or dural tear
- Hardware problems (breakage, loosening) or need for revision surgery
- Nonunion (pseudarthrosis) where bones do not fully fuse
- Continued pain or limited relief
- Adjacent segment wear above or below the fusion
- Anesthesia-related risks
Contraindications
- Active local or systemic infection
- Uncontrolled medical conditions that make anesthesia unsafe
- Severe osteoporosis that cannot support implants
- Inability to follow post-operative restrictions or care plan
- Ongoing nicotine use that cannot be modified, which may hinder fusion (relative)
Recovery Timeline
What to expect during your recovery
Most people spend a few days in the hospital and increase walking over the first weeks. Bone fusion strengthens over several months, with activity added gradually under clinical guidance.
Typical Range
90–365 days
Return to Work
28–180 days
Recovery Milestones
Sit, stand, and walk short distances with assistance in the hospital
Increase walking at home and perform basic self-care with precautions
Resume light household tasks; consider return to desk work if cleared
Begin or advance outpatient physical therapy and longer walks
Gradual return to heavier tasks and sports when approved
Frequently Asked Questions
Common questions and expert answers about this procedure
What is the goal of lumbar spinal fusion?
What is the goal of lumbar spinal fusion?
To reduce painful motion and stabilize the spine when there is instability, deformity, or damage that has not improved with non-surgical care.
How is the surgery performed?
How is the surgery performed?
Under general anesthesia, the surgeon places bone graft between vertebrae and uses implants such as screws, rods, or cages. Approaches may be from the back, front, or side.
Will fusion limit my movement?
Will fusion limit my movement?
The fused levels no longer move. Most people can do daily activities, but some bending and rotation may feel stiffer. Nearby levels may take on more motion.
How long is the hospital stay?
How long is the hospital stay?
Many people stay 2 to 4 days, depending on the approach, pain control, and mobility progress.
Will I need a brace or physical therapy?
Will I need a brace or physical therapy?
Some surgeons use a brace and most people do physical therapy. The plan depends on the surgical approach and healing progress.
What are the bone graft options?
What are the bone graft options?
Bone can come from your pelvis (autograft), donor bone (allograft), or synthetic substitutes. Each option has benefits and trade-offs.
Are the screws and rods permanent?
Are the screws and rods permanent?
Implants usually stay in place. They may be removed in select cases if they cause problems after the bone has fused.
References
Medical literature and sources