The No Surprises Act (NSA), enacted in 2022, was a historic reform intended to shield patients from unexpected medical bills arising from involuntary out-of-network care. Early data confirms the law’s initial success, with analyses showing it has over two million dollars of potential surprise billing incidents, particularly in emergency settings and for ancillary services like anesthesia at in-network hospitals. However, two years into its implementation, the law’s protections are being tested by persistent structural loopholes and a procedural mechanism that is threatening to increase systemic healthcare costs for all Americans.
Key Findings and Data Analysis
The most significant challenge to the NSA is the unprecedented volume and outcome of the Independent Dispute Resolution (IDR) process. The IDR was created as a mechanism for providers and insurers to settle payment disagreements without involving the patient. Federal regulators had projected a manageable annual caseload; however, recent data from 2024 indicates that providers initiated approximately 1.5 million disputes, exceeding initial predictions by more than 70 times. Furthermore, this data reveals a disturbing trend: arbitrators often select the higher payment offer, with 85 percent of disputes being decided in favor of the provider.
This means that in many resolved cases, the final payment exceeded the Qualifying Payment Amount (QPA)—which is tied to the median in-network negotiated rate—resulting in higher median payments. In some periods, the median winning offer was over four times the median in-network rate, suggesting that the IDR process, intended to be a neutral arbiter, may be unintentionally driving up the baseline cost of care.
The Common Scenarios That Lead to Out-of-Network Bills
While the NSA effectively banned balance billing in core situations, the threat of unexpected costs persists through specific carve-outs and nuances in provider billing practices.
- Ancillary Services at In-Network Facilities: Before the NSA, patients visiting an in-network hospital could still be billed by out-of-network providers for services like radiology, pathology, or anesthesiology. The law addressed this, but providers can still seek to bypass protections for certain scheduled, non-emergency services by requiring a patient to sign a consent form that waives their NSA rights.
- Ground Ambulance Gaps: The federal NSA explicitly does not cover ground ambulance transportation, which is a common source of high, unexpected bills, especially in emergency scenarios. While some states have implemented their own protections, a patchwork of laws leaves many consumers vulnerable to these charges.
- High Deductible Shock: The law protects consumers from charges beyond their plan’s in-network cost-sharing (e.g., copays, deductibles). Patients with high-deductible plans may still receive a large bill that is entirely appropriate under their plan design, but the unexpected size of the bill—for what they assumed was covered care—can still feel like a surprise.
Loopholes and Gray Areas in Federal and State Legislation
The primary systemic vulnerability lies in how the IDR process is being utilized by a small subset of the provider industry. Reports indicate that a significant majority of the high-volume IDR cases are filed by just a handful of large practice management, revenue management, and physician staffing corporations (Families USA, 2024). This suggests a strategic, corporate effort to exploit the arbitration mechanism to secure higher payments than the median in-network negotiated rate—the intended benchmark for the QPA.
Furthermore, the complexity of the law has led to compliance issues on the payer side. Federal enforcement actions have cited insurers for issues such as the inaccurate calculation of the QPA (LUGPA Policy Update). Since the QPA is the foundational figure in the IDR process, any manipulation or error in its calculation can corrupt the entire system and undermine the goal of fair market prices.
The Financial Burden on Patients and The Push for Further Reform
The true cost of the IDR logjam extends beyond the administrative burden on regulators. When arbitrators consistently award providers payments substantially higher than the median in-network negotiated rate, the increased costs are ultimately absorbed by the system and passed on to all consumers in the form of higher premiums. This effectively undermines the cost-saving intent of the original legislation.
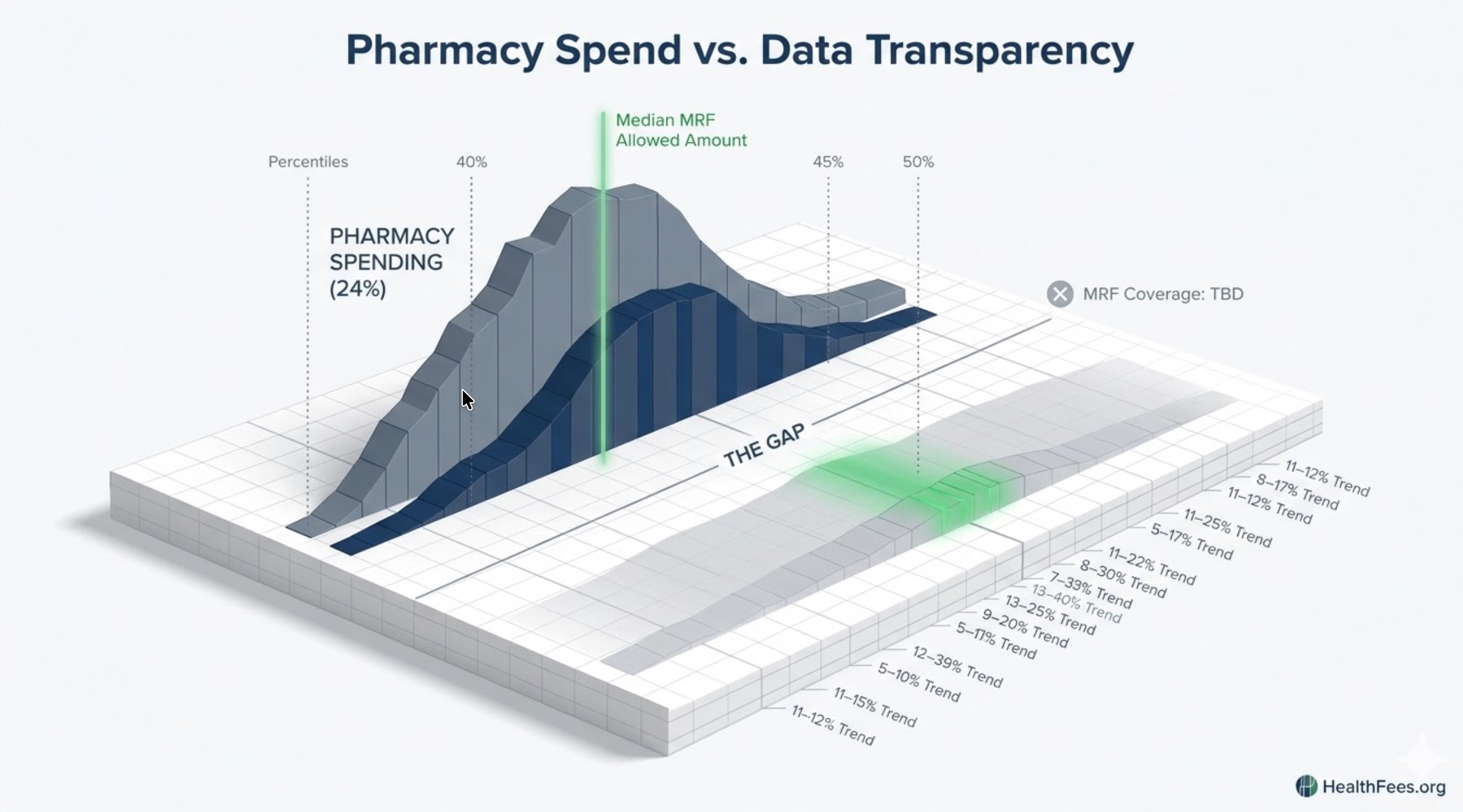
Addressing this systemic issue requires more than just improving the IDR process; it demands deeper transparency. The release of mandated insurer and provider pricing data, including both in-network negotiated rates and out-of-network allowed amounts, is essential for analysts to monitor these trends and verify compliance with the QPA standard.
Systemic Implications and Outlook
The ongoing challenge with out-of-network charges highlights a critical flaw in the market: price is still not primarily determined by value or competitive forces, but by negotiation leverage and the strategic exploitation of regulatory gray areas. The data from the IDR process provides a unique window into the true price floor for certain services, demonstrating the wide gap between what providers charge, what insurers prefer to pay, and the actual cost of the service.
The push for full healthcare price transparency—making all payer rates public and accessible—gains momentum as the IDR issues continue. Only by arming researchers and policymakers with complete, verified datasets can the market be disciplined enough to reduce price variation and ensure the protections guaranteed by the NSA are not compromised by procedural abuse.
Conclusion: The Takeaway
The fight against unexpected medical bills is not over. While patients are largely protected from being sent a surprise bill, the underlying system of payment negotiation is under significant strain from high-volume, corporate disputes that are inflating costs for everyone. The long-term success of healthcare price reform rests on the ability of regulators and consumer watchdogs to monitor the integrity of the data—specifically the negotiated rates and allowed amounts—that form the foundation of the law.